
Medical history is important. It gives us a framework of where we have been and where we need to go. It shapes the way we think and practice medicine but also guides our future.
The history and intersection of Turner syndrome (TS) and Diabetes Mellitus (DM) can give us valuable insight into current research gaps and ways to improve longitudinal care. Read more to explore the history and current findings of TS and DM.
The information in this blog is based on a webinar presented by Dr. Catherina Pinnaro, “Diabetes: Diagnosis, Management, and Research.”
What is Diabetes Mellitus?
Diabetes mellitus is a chronic metabolic disorder characterized by high blood sugar (hyperglycemia) resulting from the body’s inability to produce or properly use insulin. Common symptoms include excessive thirst, frequent urination, fatigue, and blurry vision.
TS carries a significantly increased risk of diabetes mellitus, with a roughly 4-fold to 11-fold higher risk than the general population. Risk increases with age, with a mean onset of 36–38 years.
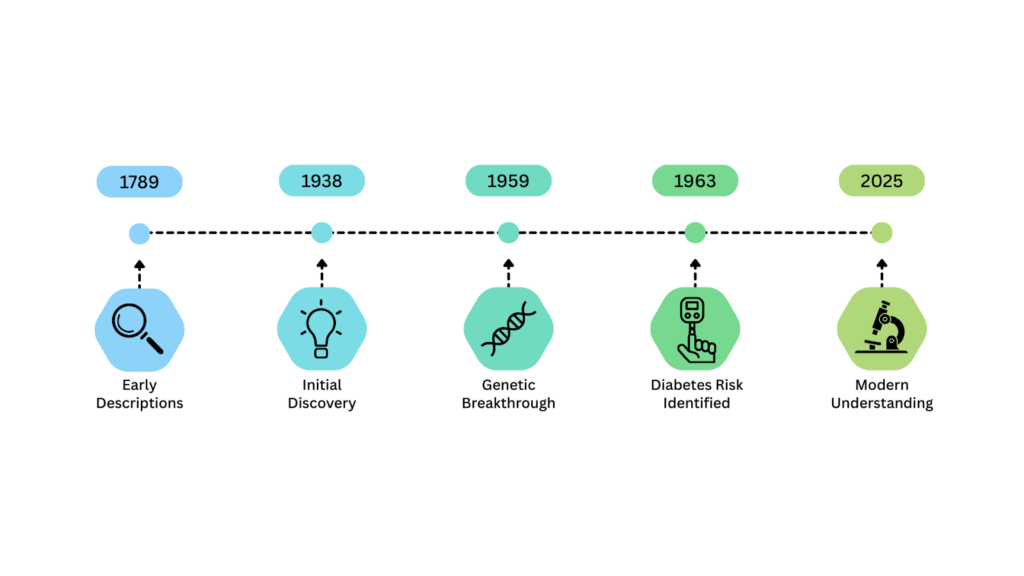
Initial Discovery: 1920s-1930s
Early descriptions of TS date back to the late 1700s, where physicians began to describe physical features that would eventually be known as Turner syndrome. In 1938, Henry Turner and Otto Ullrich were the first to document and publish their findings of TS. They described characteristics like short stature and underdeveloped ovaries but they did not notice a higher incidence of diabetes or metabolic disease within the population.
Genetic Breakthrough: 1950s
In 1959, a crucial finding changed our understanding of TS from physical and reproductive characteristics to genetic etiology. Charles Edmund Ford noted that TS can be attributed to an absent second X chromosome. This breakthrough allowed scientists to begin questioning why specific characteristics and potential metabolic risk factors, like diabetes mellitus, can occur in TS.
Diabetes Risk Identified: 1960s
In 1963, Forbes and Engel recognized a higher risk of diabetes in Turner syndrome. In a specific study, TS was grouped in a category called Gonadal Dysgenesis, which is a group of disorders resulting from underdeveloped gonads (ovaries or testes). When participants drank a sugary drink, their blood glucose (sugar) increased more than expected. It was found that the individuals in this study had “chemical diabetes.” They had no symptoms or signs but it highlighted the link between TS and irregular glucose metabolism.
Modern Understanding
Today, our understanding of diabetes in Turner syndrome does not fit into the common classification of Diabetes Mellitus Type 1 or Type 2. Some researchers have referred to it as Type 3 or TS-specific Diabetes. In several studies, the loss of the X chromosome in women with TS has been shown to contribute to the higher rate of glucose abnormalities and demonstrated impaired insulin secretion or release.
Impaired glucose tolerance is common in Turner syndrome. The risk of Diabetes Mellitus in TS is 4-11 times higher than in women with two X chromosomes, (46,XX). The risk of glucose intolerance increases with age in Turner Syndrome, so it is important to begin testing early. There is a correlation between increasing BMI (body mass index), but obesity is not the primary factor.
Management of Turner Syndrome and Diabetes Mellitus
There are several treatments that are commonly used for individuals with Turner syndrome, and you may be wondering how they impact diabetes risk.
- Growth Hormone (GH) has been shown to worsen insulin resistance but its long term use does not increase the risk of diabetes.
- Estrogen can help overall metabolic processes but its effect on glucose tolerance is not clear.
- Oxandrolone is a steroid that is used along with GH and estrogen replacement and it’s unclear whether that has any effect on glucose tolerance.
Why screen for Diabetes Mellitus?
High blood sugar can damage blood vessels over time, resulting in chronic complications. It can have lasting effects on the eyes and kidneys and even results in heart attacks and strokes. Since DM can be asymptomatic in individuals with TS, it is important to screen for DM starting at 10 years old.
Blood tests to check blood glucose and hemoglobin A1C should be done every year. It is important to note a low A1C test does not always indicate that someone does not have DM. We should be using a combination of A1C tests, blood glucose measurements, and Oral Glucose Tolerance Testing (OGTT) to detect diabetes.
Despite decades of research on Turner Syndrome and Diabetes Mellitus, there still remains large gaps in our screening and management. By studying history, we are reminded how far we have come and how much further we need to go. Continued research and individualized care will help improve long-term outcomes and support the TS community.
Additional Resources

References
Mitsch, Cameron, et al. “Hyperglycemia in Turner Syndrome: Impact, Mechanisms, and Areas for Future Research.” Frontiers in Endocrinology, U.S. National Library of Medicine, 15 Feb. 2023, pmc.ncbi.nlm.nih.gov/articles/PMC9974831/#s4.
Sun, Lin, et al. “Glucose Metabolism in Turner Syndrome.” Frontiers, Frontiers, 18 Feb. 2026, www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2019.00049/full.
Written by Simrita Hemrajani, TSF Volunteer Blog Writer.
