

Turner Syndrome patients have an increased risk for several skeletal issues, including knock knees, also known as genu valgum. Knock knees have significant implications for mobility and long term joint health, but can be treated most effectively with early diagnosis. Thus, this article focuses on knock knees in individuals with TS, covering prevalence, potential impacts, treatment options, and the importance of early intervention.
What are knock knees?
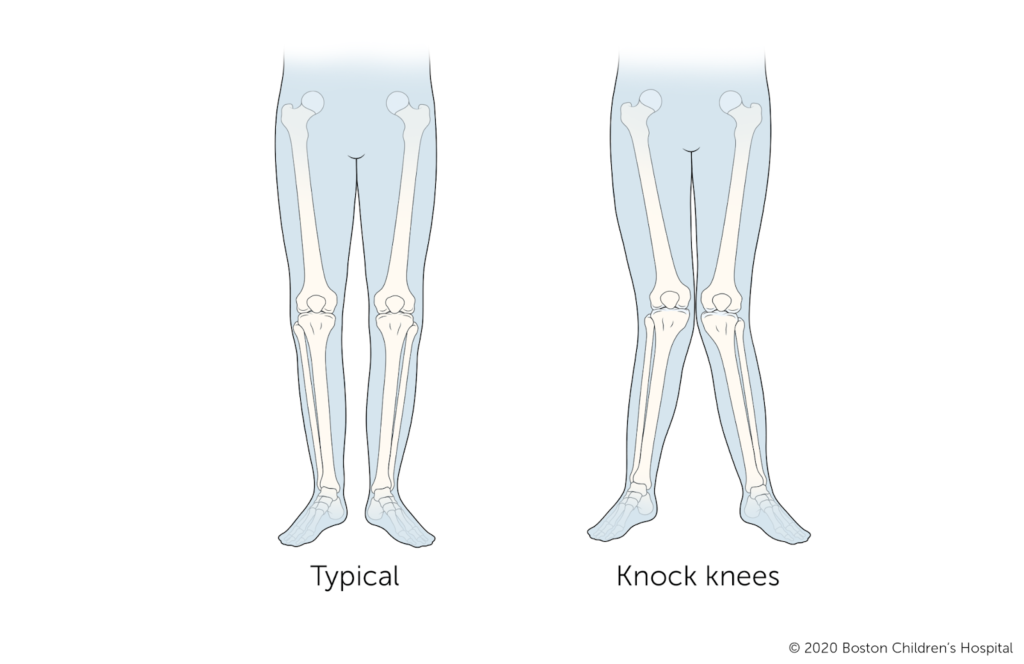
Knock knees, also known as genu valgum, is a condition in which the knees angle inward when the legs are straightened, with ankles unable to touch (NHS, 2025).
Individuals with TS are most likely to have idiopathic genu valgum, which refers to knock knees resulting from congenital or unknown causes, rather than normal development (NHS, 2025).
Prevalence of Knock Knees in Individuals with TS
Anecdotal evidence of a high prevalence of knock knees in individuals with TS is supported by a 2011 study of 62 individuals with TS that found over 60% were affected with knock knees (Trzcińska et al., 2011). This correlation is likely to be highly genetic, and specifically related to the SHOX gene.
The SHOX is a gene located on both sex chromosomes, meaning patients with TS often have only one copy, which may not produce enough protein to fully carry out its normal function (Acosta et al., 2019).
SHOX regulates longitudinal bone growth, and mutations in this gene can cause short stature and other skeletal issues in individuals without TS as well (Acosta et al., 2019).
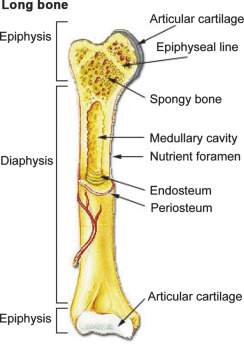
Usually, SHOX is expressed in the cells that form the perichondrial layer, which is essential for endochondral ossification, the process in which most bones develop from a cartilage scaffolding (Dwek, 2010). This process is especially condensed in the diaphysis, or main shaft, of long bones including the radius, ulna, tibia, and fibula (Dwek, 2010). Therefore, individuals with insufficient SHOX gene may experience bowing or shortening in these regions that can lead to short stature, turned in elbows, and knock knees.
Impact of Knock Knees
Knock knees cause an increased load on one or both knees, which can cause pain and further injury to the knee, as well as progressive degeneration of the knee joint. In untreated adults, the imbalance of force on the outside and inside of the knee can lead to chronic pain, instability, and arthritis (Hospital for Special Surgery, 2025).
It can also lead to reduced range of motion in hips and difficulties walking or running (Hospital for Special Surgery, 2025).
Diagnosis of Knock Knees

Healthcare providers can diagnose knock knees with a physical examination of a patient’s gait (Patel & Nelson, 2023). In some cases, a radiograph may be required to confirm the diagnosis based on measurement of the tibiofemoral angle (indicated by the asterisk (*) in the image below) (Patel & Nelson, 2023).
Image source: Comparison of the Clinical Outcomes (Note that this image is intended to illustrate the location of the tibiofemoral angle and is not an example of knock knees).
It is recommended to seek the opinion of a healthcare professional if you or your child appear to have knock knees. This can be indicated by the following symptoms (NHS, 2025):
- A gap between the ankles of more than 8cm when standing with knees together
- 1 or both knees being painful, swollen, stiff, or warm to the touch
- Different lengths of legs
- Limping or difficulty walking
Early diagnosis is essential for knock knees, since the younger a patient is, the more rapidly a treatment will take effect.
Treatment of Knock Knees
The most common treatment for knock knees in patients who are not skeletally mature is guided growth with hemiepiphysiodesis. This is a minimally invasive surgical procedure that uses a surgical implant to guide the growth of the tibia and femur into better alignment (Patel & Nelson, 2023).
Once an individual has fully matured, the treatment for knock knees is an osteotomy, a more invasive procedure that involves surgically cutting or reshaping the bone to correct its angle (Patel & Nelson, 2023).
Depending on severity, many cases of knock knees do not require any of these interventions, so it is essential to consult with a healthcare professional upon diagnosis to determine the most appropriate next steps for each individual.
Conclusion
Knock knees cause an imbalance in the lower body that not only be painful, but also have significant implications for mobility and arthritis risk later in life. Due to the genetic causes of knock knees, individuals with TS are more likely to develop the condition. \
Being aware of the symptoms and raising any concerns with a healthcare provider can ensure that any incidence of knock knees can be promptly diagnosed and treated early, when intervention is the most successful.
References
Acosta, A. M., MD, Steinman, S. E., MD, & White, K. K., MD, MSc. (2019). Orthopaedic manifestations in Turner syndrome. In American Academy of Orthopaedic Surgeons, Journal of the American Academy of Orthopaedic Surgeons (pp. e1021–e1028) [Journal-article].
Dwek, J. R. (2010). The periosteum: what is it, where is it, and what mimics it in its absence? Skeletal Radiology, 39(4), 319–323.
Hospital for Special Surgery. (2025, January 3). Knock knee.
Knock Knees | Boston Children’s Hospital. (n.d.).
Kwak, J., Jeong, J., Lee, S., Jung, H., & Jung, Y. (2012). Comparison of the Clinical Outcomes after Total Knee Arthroplasty with the LCS Rotating Platform Mobile Bearing Knee System and the PFC Sigma RP-F Mobile Bearing Knee System. Clinics in Orthopedic Surgery, 4(4), 256.
NHS. (2025, May 22). Knock knees. nhs.uk.
Patel, M., & Nelson, R. (2023, May 29). Genu valgum. StatPearls – NCBI Bookshelf.
Trzcińska, D. (2011). The knee alignment and the foot arch in patients with Turner syndrome. PubMed.

![]()
